
IMAGINE Impact Stories: How the IMAGINE Network is leading the way in quality care, policy, and knowledge translation.
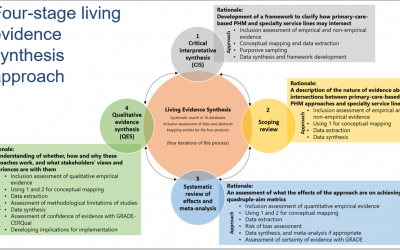
Advancing a living evidence synthesis about the intersections between primary-care based population-health management (PHM) approaches and specialty service lines
Preventing and managing chronic conditions – such as inflammatory bowel disease (IBD) and irritable bowel syndrome (IBS) – is a key challenge for health systems across Canada. Many patients who are at risk of developing IBD/IBS or other chronic conditions are not...
Digital Tools for IBS
Irritable bowel syndrome (IBS) is a chronic condition that significantly affects patients' quality of life. Managing IBS is complex, involving both physical and psychological symptoms that can be difficult to control. Digital health interventions (DHIs) have the...
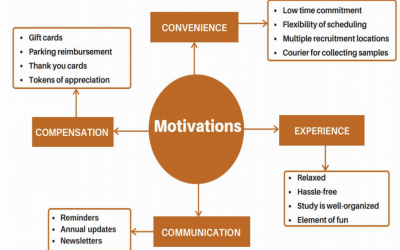
An innovative patient-led patient-oriented qualitative research project to understand the motivations and barriers to getting and staying involved in IMAGINE’s MAGIC study – Implementation Phase – (completed September 2020)
The IMAGINE Network’s main research study, MAGIC, is a large longitudinal national cohort study investigating the interactions between inflammation, microbiome, diet and mental health in patients with inflammatory bowel disease(IBD) and irritable bowel syndrome (IBS)....

Fecal Microbial Transplantation in active Ulcerative Colitis with Antibiotic Pre-treatment – Analysis Phase – October 2020
Ulcerative colitis affects approximately 80,000 Canadians and is thought to arise from a disordered immune response to gut contents in predisposed individuals. Current therapies for UC remain expensive and imperfect with 50% of patients needing hospitalization and...

Supporting Rapid Learning and Improvement for Select Chronic Conditions in Canada (final results completed February 2020)
Adopting a problem-focused rapid-learning and improvement orientation in health systems presents an opportunity for constant and iterative improvements in patient care and experiences across a number of chronic conditions. Rapid learning can take place at all levels...
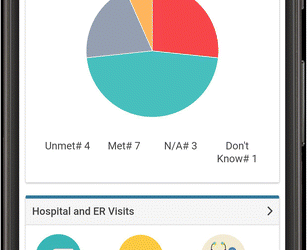
Patient Monitoring App for IBD (completed Jan 2021)
Through IMAGINE’s partnership with Crohn’s and Colitis Canada, the PACE Health Services research projects (Telemedicine for IBD; HealthPROMISE Patient Monitoring App, Quality Indicators in IBD Care; and e-Clinical Care Pathways to reduce steroid use) continue to...

Raising Profile of Patient Voice in Healthcare Decision-Making (On-going)
Our Network’s Principal Investigator, Dr. Paul Moayyedi, was appointed Co-ordinating Editor of Cochrane Gut back in June 2020. Cochrane Gut aims to use evidence from randomised controlled trials to answer practical questions on the diagnosis, prevention, treatment,...
RECRUITMENT AND RETENTION PROJECT IMPLEMENTATION (Implementation completed June 2021, Evaluation on-going)
As reported in our last year’s annual report, our Network supported an innovative patient-led patient-oriented qualitative research project to understand the motivations and barriers to getting and staying involved in IMAGINE’s main research study, MAGIC study. Given...

Canadian Clinical Practice Guidelines for the Management of Irritable Bowel Syndrome (IBS)
Irritable Bowel Syndrome (IBS) is a common gastrointestinal disorder that affects approximately one in 10 individuals in North America. IBS imposes a significant burden on the health care system and reduces quality of life. Recently, both the Canadian Association of...

Policy KT Project: Reducing Emergency-department Usage in People with Inflammatory Bowel Disease in Provincial Health Systems in Canada (January 2019)
Canada has one of the highest rates of inflammatory bowel disease (IBD) in the world, affecting approximately one in every 150 Canadians. Given the burden of IBD and complications associated with its care, there is a high utilization of emergency department healthcare...

PACE Program: Telemedicine for IBD Care
No matter where a patient lives, it is essential that they can access their healthcare team. Early disease detection and timely IBD care can improve overall quality of life, and reduce the need for invasive and expensive surgeries. However, there is significant...
